THE WINNER IS SABRINA TAYLOR

Congratulations to Sabrina Taylor who has won the student essay competition.
Sabrina Taylor is a 21-year-old medical student at University College London Medical School with an additional iBSc (Hons) Oncology degree. Her interests in global health and medical education have translated into her winning essay on discussing the long-term impacts of the COVID-19 pandemic on various elements of global health provisions. She hopes her essay will serve as a platform to encourage other students to gain an interest in important healthcare affairs outside the medical curriculum and initiate conversations about lessons learnt from a global healthcare crisis.
Comments from the judges included that Sabrina’s entry was as good as most of the articles in the medical editorial columns.
Please find Sabrina’s excellent essay below.

THE RUNNERS-UP
Lissa Darby
Congratulations to Lissa Darby who is one of our two runners-up.
Lissa Darby is going into her penultimate year of graduate entry medicine at the University of Southampton. She has been interested in global health since completing a volunteer placement in Tanzania during her gap year, so is delighted to have won a prize in a subject she is so enthusiastic about. Once qualified, Lissa hopes to pursue her learning in global health, obtain training in tropical medicine and eventually work abroad with organisations to improve healthcare where it’s needed most. In the meantime, she’s looking forward to her upcoming clinical placements in Jersey and the beaches that await there!
Lissa says “I’m grateful for the opportunity to take part in this competition and hope you enjoy reading the essay as much as I enjoyed researching and writing it.”
Please enjoy Lissa’s essay.
Innovation and implementation of new technologies to improve global health is a compelling example of the value and necessity of collaboration between different disciplines to achieve optimum healthcare provision. Just as members within a team must communicate effectively, so must health services be connected to those that use them. One of the major challenges in attaining widespread healthcare to meet the human rights of all populations (1) in low and middle-income countries is access by rural communities to healthcare provisions, and vice-versa. Geographical, financial, and infrastructural factors combine to create often insurmountable barriers to healthcare and generate massive health inequalities between those living in urban and rural areas. Recently, the use of unmanned aerial vehicles (UAVs), or drones, has been an important focus of research and innovation to overcome these obstacles. This essay will explore the use of UAVs and their potential to significantly improve healthcare in low- and middle-income countries (LMICs).
The Need
A World Bank and World Health Organisation (WHO) report in 2017 stated that at least half of the world’s population is unable to access essential health services (2). The United Nation’s (UN) 2019 political declaration following a meeting discussing universal health coverage states that current progress to achieving the health sustainable development goal by 2030 is inadequate (3). A report by the Global System for Mobile Communications Association (GSMA) found that service delivery and infrastructure and supplies are some of the biggest healthcare challenges in developing countries (4).
In Rwanda less than 20% of roads are paved, creating a massive hindrance to timely delivery of medical supplies and transfer of specimens to test facilities (5). UNICEF’s HIV/AIDS unit in Malawi identified a significant factor impeding early infant diagnosis of HIV was the inefficient connection between the nine testing laboratories and the 650 units providing paediatric HIV services. Like many countries, transport of samples in Malawi relies heavily on motorbike couriers. However, its efficiency is inevitably limited by human factors and poor road infrastructure (6).
Limited access to vaccines has a painfully stark impact on human life. In the Democratic Republic of Congo (DRC), for example, vaccine-preventable diseases kill 1 in every 7 children under the age of 5. Furthermore, UNICEF found that only around a third of children are fully vaccinated in their first year of life, and that more than 150,000 children in the DRC did not receive a single dose of vaccines such as those against polio, tetanus and whooping cough (7).
Van Olmen et al. recommend primary care facilities should be within 5km or 1 hour’s walk of populations and that secondary care centres should be available at the ratio of 1:100,000 people. If these recommendations are not met, the demand is simple: provide new facilities, or improve the method of access either by increasing transport or improving road quality (8). Drones provide an added tool with which to address these issues.
The role of UAVs in improving health provision globally is significant, varied and could improve all aspects of healthcare, from delivering blood for emergency transfusions to collecting specimen samples from patients at home. They can also be used to map areas affected by recent natural disasters to assess damage and plan emergency responses, or to disinfect areas affected by viruses, as during the COVID-19 pandemic in countries like India and Sri Lanka (9).
Current work
Various private companies have been working closely with governments in LMICs to establish the need and potential for use of UAVs. One collaborated with the Government of Vanuatu, where an estimated 1 in 5 children do not receive their essential childhood vaccinations due to geographical barriers, to deliver the world’s first drone-delivered vaccine to a one-month old baby (10).
Following this success, the same company ran a larger trial programme in the DRC in July 2020 delivering vaccines, syringes and drugs to a village a three-hour drive from the distribution centre. The drones completed the journey in 20 minutes, enabling two months’ worth of supplies to be provided to health facilities in a fraction of the time possible by road. Furthermore, the UAVs were loaded with blood samples to be tested and were able to return these within the strict time limits of biological sample testing (11). Expediating delivery of supplies for vaccination will increase uptake for vaccination programmes and enhance protection of populations against various infectious diseases. This is especially important in rural communities, where access to treatment for vaccine-preventable diseases may be non-existent compared to urban areas.
Another private company has worked with the government of Rwanda to establish an emergency delivery-by-drone service that allows doctors to order blood products by text message. The blood is then delivered by parachute with an average delivery time of 30 minutes. Rabies vaccines, which must be administered as soon as possible after the bite is sustained, can also make up the UAVs’ cargo (12). Throughout the COVID-19 pandemic this company also exploited their existing technology to address needs created by the devastating pandemic. In Ghana, for example, UAVs were used to overcome issues arising from restrictions on movement and physical human contact due to the coronavirus by delivering medical supplies by parachute (13). Democracy was also protected using UAVs, despite the world-stopping pandemic, as UAVs delivered emergency personal protective equipment (PPE) to polling stations. The task was carried out in half the time and moreover, it was estimated that twice as much PPE was distributed compared to conventional road methods. Here the use of UAVs allowed the election to proceed safely, which would otherwise have been impossible (14).
In 2017 in Malawi, UNICEF established a ‘drone corridor’ and worked with local authorities to encourage businesses and universities to run trials delivering medical supplies and collecting blood samples via UAV (6). Not only did this encourage innovation and investment in the local area, but now, two years later, deliveries sometimes taking up to six weeks are completed in half the time and the projects are expanding (15). Kazakhstan was another country to recognise the potential of UAVs improving access to healthcare and has become the location for two more test corridors established alongside UNICEF’s Office of Innovation (6).
Rural areas in the developed world have also benefited from the use of UAV deliveries, as parts of North Carolina became the first locations to receive medical products and PPE via drone delivery following an emergency waiver granted by the United States Federal Aviation Administration. Different companies based in the United Kingdom have similarly successfully expediated provision of medical supplies to parts of Ireland and of the Isle of Wight (16).
Considerations
A significant factor potentially limiting the widespread implementation of the transport of medical supplies via UAVs, is the initial cost. Several costing studies have found the use of UAVs to be less cost-effective than using motorcycles, the most commonly used method for this task (9). However, it is likely that as drone technology develops and production expands costs will reduce. Furthermore, the long-term economic savings of delivering better healthcare to a population are difficult to determine but will possibly make the initial higher investment worthwhile.
As with any new, automated technology there is apprehension of the machine ‘replacing’ humans in their work. The motorcycle courier component of the supply chain, currently essential in so many countries, represents an important source of employment for many people in rural areas where secure employment may otherwise be hard to obtain. Of course, implementation of UAV networks in these areas will require a workforce, but this may demand an entirely different skillset to that held by many local residents. This provides opportunity for training and development of skills among a population. However, initial stages of establishing these new service networks will necessitate a significant time investment into training, or may present the “risk” of outsourcing skills from other areas or countries.
The use of UAVs significantly increases speed of transport time. However, to achieve maximum efficiency the speed of lab testing, for example, must match these improvements. The true extent of the benefit of using drones will only be felt if facilities receiving samples have the capacity to keep up with increased delivery rates. The same is true for stock capabilities. There may be a significant need for improvement of many aspects of health infrastructure alongside the introduction of faster transport services to maximise the advantages therein.
Finally, a significant barrier to the use of UAVs is government policy. Drones have long been associated with military action, surveillance, and underhand activity, so their use is often met with suspicion. Regulating UAVs is relatively new territory so authorities may be hesitant to engage with it. Significant restrictions in the US have hindered many companies’ progress in developing their UAVs, which has led to many seeking permissions abroad (17). Many rural areas of LMICs have benefited from this, as in the work of private companies described above. It has also led to these countries’ governments becoming innovators in terms of UAV regulations (9).
Conclusion
Improving healthcare of populations not only has a benefit on a humanitarian level, but also contributes hugely to the development of countries’ economies and their participation on the world stage. In a rapidly changing world – and one so recently drastically changed by the force of a devastating pandemic – innovative solutions are a necessity to achieve and maintain sustainable equality in people’s livelihoods. As a global society we are faced with challenges of climate change and a growing population, both of which are significantly impacting global health. Now more than ever reliable and fair access to health services is essential and the investment in new technologies such as UAVs would optimise this.
The potential gains from the use of UAVs in developing countries to enhance access to healthcare are enormous. There are countless examples of improvements being made to people’s lives through the increased efficiency of delivery of medical supplies and of transport of test samples. Innovative companies and organisations have made huge advances in their UAV technology to make them suitable for this purpose. Drones with the capacity to refrigerate vaccines and biological products are already in use, and their creators have optimised their services to include storage, as well as launch and landing facilities that can be rapidly assembled and easily run to facilitate their implementation (18).
On the other hand, establishing these networks in rural areas may require significant initial financial investment and the long-term cost-benefit compared to existing transport services is yet to be established. On-the-ground training and education is essential to ensure acceptance of the new technology and to ensure its maximum potential is reached. Furthermore, other components of the healthcare supply chain and medical service infrastructure must be optimised to make services maximally efficient and beneficial to those who need it.
Clearly, more work and time is needed to fully assess the role of UAVs in optimising health services in LMICs but advances thus far are promising. Continued investment and engagement alongside inclusive, discursive, and altruistic collaboration of innovators with health service providers can repurpose this technology initially developed for military use to instead improve and save millions of human lives.
References
- WHO Constitution [Internet]. 1946 [cited 2021 May 30]. Available from: https://www.who.int/about/who-we-are/constitution
- Gabriela Flores, Daniel Hogan, Gretchen Stevens, Justine Hu, Tessa Tan-Torres Edejer, Sarah Thomson, et al. Tracking universal health coverage: 2017 global monitoring report. [Internet]. World Health Organization and International Bank for Reconstruction and Development / The World Bank; 2017 [cited 2021 May 30]. Available from: https://documents1.worldbank.org/curated/en/640121513095868125/pdf/122029-WP-REVISED-PUBLIC.pdf
- Political declaration of the high-level meeting on universal health coverage [Internet]. United Nations General Assembly; 2019 Sep [cited 2021 May 30] p. 3. Available from: https://undocs.org/en/A/74/L.4
- Sam Ajadi. Digital Health A health system strengthening tool for developing countries [Internet]. Global Systems for Mobile Communications Association; 2020 [cited 2020 May 30]. Available from: https://www.gsma.com/mobilefordevelopment/wp-content/uploads/2020/11/Digital-Health-June-2020.pdf
- Brian McManus. How Rwanda Built A Drone Delivery Service [Internet]. Real Engineering; 2019 [cited 2021 May 28]. Available from: https://youtu.be/jEbRVNxL44c:
- Drones for Delivering Results for Children [Internet]. UNICEF; 2019 Nov [cited 2021 May 31]. Available from: https://www.unicef.org/evaluation/media/936/file/Drones%20for%20Delivering%20Results%20for%20Children.pdf
- DRC’s First Medical Drone Vaccination Program [Internet]. Swoop Aero. 2021 [cited 2021 May 31]. Available from: https://swoop.aero
- Van Olmen J, Criel B, Van Damme W, Marchal B, Van Belle S, Van Dormael M, et al. Analysing health systems to make them stronger. Antwerp, Belgium: ITGPress; 2010.
- Are drones suitable tools for delivering medical supplies in developing countries? [Internet]. Mobile for Development. 2020 [cited 2021 May 30]. Available from: https://www.gsma.com/mobilefordevelopment/blog/are-drones-suitable-tools-for-delivering-medical-supplies-in-developing-countries/
- The world’s first two-way medical drone logistics network in Vanuatu [Internet]. Swoop Aero. 2018 [cited 2021 May 30]. Available from: https://swoop.aero
- Swoop Aero commences medical drone deliveries in DR Congo [Internet]. Medium. 2019 [cited 2021 May 30]. Available from: https://medium.com/@swoop_aero/swoop-aero-commences-medical-drone-deliveries-in-dr-congo-6b3e1a7f81ad
- Using drones to deliver blood in Rwanda. BBC News [Internet]. 2019 Mar [cited 2021 May 31]; Available from: https://www.bbc.co.uk/news/av/business-47631709
- Zipline delivers over 1 million vaccine doses to hard-to-reach areas of Ghana [Internet]. GhanaWeb. 2021 [cited 2021 May 31]. Available from: https://www.ghanaweb.com/GhanaHomePage/NewsArchive/Zipline-delivers-over-1-million-vaccine-doses-to-hard-to-reach-areas-of-Ghana-1171270
- Protecting Ghana’s Election: Instant Agility With Zipline’s Autonomous Delivery Network [Internet]. zipline.com; 2021. Available from: https://assets.ctfassets.net/pbn2i2zbvp41/3yrQaMNdJ1u1J2aSEucjzt/4412ea5d12896d15b7eb41a2212d0295/Zipline_Ghana_PPE_Global_Healthcare_Feb-2021.pdf
- Malawi drone initiative takes drugs to remote areas faster. Financial Times [Internet]. 2019 Nov 29 [cited 2021 May 31]; Available from: https://www.ft.com/content/aab0945c-f62c-11e9-bbe1-4db3476c5ff0
- Zipline drones deliver supplies and PPE to US hospitals. BBC News [Internet]. 2020 May 27 [cited 2021 May 31]; Available from: https://www.bbc.com/news/technology-52819648
- Renee Knight. Drones Deliver Healthcare [Internet]. dronesinhealthcare. 2017 [cited 2021 May 30]. Available from: https://www.dronesinhealthcare.com
- Zipline – Vital, On-Demand Delivery for the World [Internet]. [cited 2021 May 31]. Available from: https://flyzipline.com/how-it-works/
Olivia Latherton

Congratulations to Olivia Latherton who is our jont runner-up.
Olivia Latherton is 19 years old and is currently doing a master’s in children’s nursing at Birmingham University and has just finished her first year.
Olivia studied Spanish, psychology and biology at A-level.
When she needs a break from studying, Olivia enjoys fitness and various forms of art.
Well done to Olivia and please find her brilliant entry essay below.
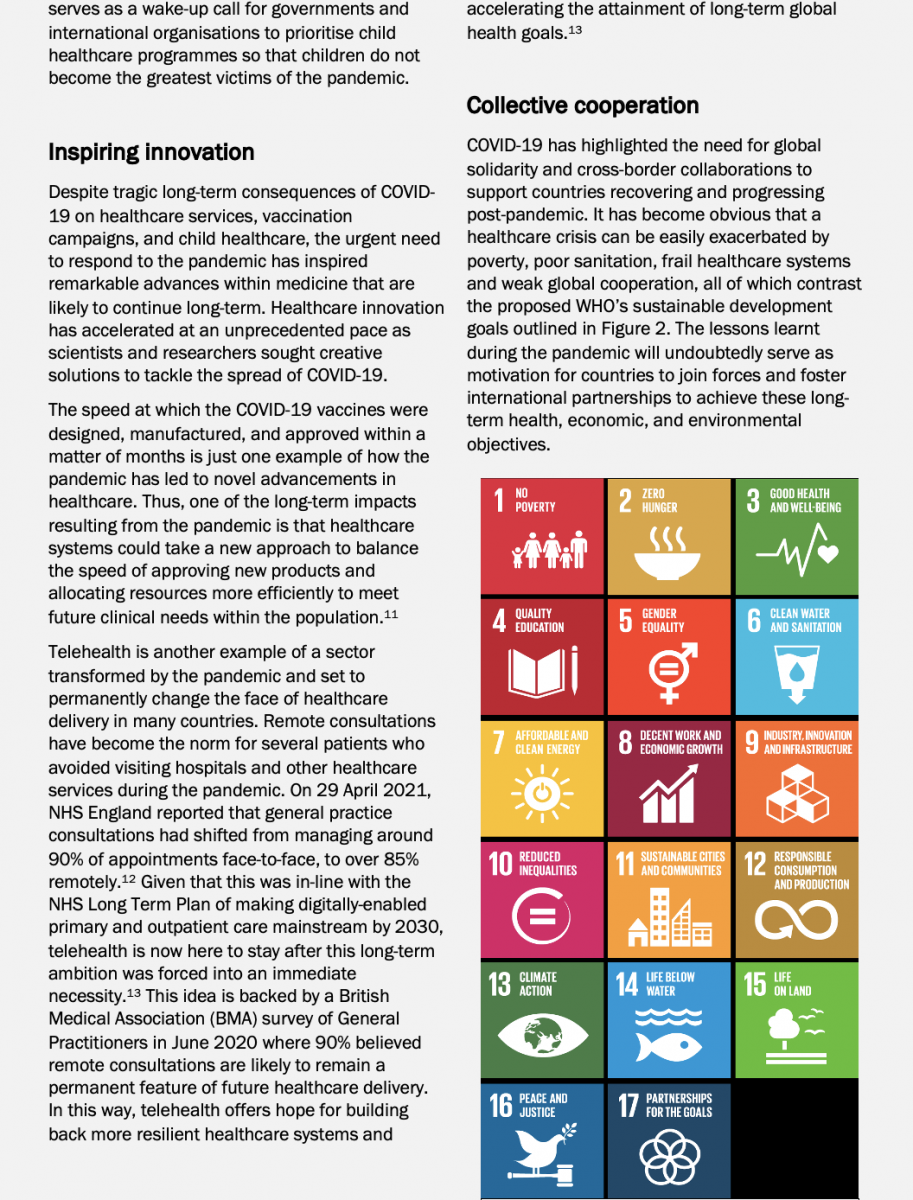
Discuss the long-term impact of COVID-19 on any element of global health provision
The global COVID-19 pandemic has profoundly impacted on society as a whole, with the number of confirmed cases reaching approximately 117 million and the number of deaths at 2.6 million as of March 10th, 2021 (JHU, 2021). As the world tries to recover from this crisis, it is important to consider the long-term consequences, especially in regard to the delivery of healthcare. Nurses are guided by a code of practice, developed by the Nursing and Midwifery Council, which aims to protect patients, ensuring their care is the priority and they are treated as individuals (Pattison et al, 2010). This is achieved through Person-Centred Care (PCC) which was devised to allow patients to play a more active role in their treatment by empowering them to be at the forefront of decision-making (McCormack et al, 2017). The approach has been instigated in many healthcare settings due to the numerous advantages it presents, as it is directly correlated to wellbeing; reduces patient fears; increases treatment compliance and cuts down on healthcare costs (Gameiro et al, 2013). This essay will consider the impact COVID-19 will have on healthcare professionals to provide effective PCC.
COVID-19 has changed the way in which society functions, with those who are not key workers having to isolate and work from home. Social media and video conferencing platforms such as Skype, Microsoft Teams and Zoom have become our primary method of communication, with Zoom seeing a 360% rise in usage since the beginning of the pandemic (Williams, 2021). In 2015, approximately two percent of employees worked remotely, however the Coronavirus outbreak caused a huge spike in this figure, with remote working becoming the norm. Whilst this study was held in China, this was reflected in other countries (Wang et al, 2021).
In an attempt to minimise direct contact and help prevent the spread of Coronavirus, numerous healthcare services have switched to telehealth appointments via phone calls or Zoom (Wosik et al, 2020). Telemedicine presents numerous benefits, as it is not only economical, cutting down on travel costs, but also increases the efficiency of appointments, increasing staff productivity (Mills et al, 2020). Nevertheless, virtual appointments also have multiple drawbacks, including limitations when undergoing physical examinations, technical challenges, issues concerning confidentiality and whether access to technology may act as a barrier to retrieving treatment (Gajarawala et al, 2021). Moreover, many patients feel these consultations are impersonal and negatively influence the continuity of care, two core principles of PCC (Kuzma, 2020).
The PCC approach attempts to deliver personalised care by putting the patient at the heart of every decision, meaning that biochemical needs are not the sole focus, leaving service users feeling valued and supported (Lehuluante et al, 2021). Telemedicine acts as a barrier to the formation of a successful partnership between the nurse and patient, with a study of rhinology patients in the US finding that 62.2% of patients prefer face-to-face appointments (Hentati et al, 2021). A study conducted by Itamura et al (2020) reported that patients attending virtual visits rated their experience much lower in many categories, including knowledge of previous medical history and ease of connection to the provider, compared to those who attended in-person. Overall, telemedicine has granted access to healthcare services during the COVID-19 outbreak that otherwise may not have been possible. However, its use acts as a barrier to PCC due to the difficulty in forming an inter-professional relationship with patients, resulting in impersonal treatment.
Face masks have become an essential part of our everyday attire, helping to reduce the transmission of coronavirus, whilst also encouraging social distancing (Angel et al, 2020). The media focused their attention on the lack of Personal Protective Equipment (PPE) available to healthcare workers, which emphasised their vulnerability to the disease. While all healthcare workers are required to wear masks, those working directly with COVID-19 patients have a wider array of PPE comprising of masks, gloves, gowns, goggles and face shields (Mahmood et al, 2020). Although a necessary precaution, the extensive use of face masks has been shown to both increase loneliness and disrupt effective communication, a crucial part of PCC, by concealing the mouth which conveys meaning behind dialogue (Campagne, 2021).
Non-verbal communication constitutes 55% of human communication compared to 7% verbal (Islam et al, 2020). Covering the mouth hinders the non-verbal expression of emotions (Carbon, 2020). Research has also shown that positive facial expressions can help reduce anxiety, which mask-wearing prevents (Mheidly et al, 2020). From the evidence we can clearly conclude that face masks inhibit the ability to communicate efficiently, a hinderance to PCC. Ferguson et al (2013) suggested the need for good communication between patients and professionals, finding that patients did not simply want information regarding their diagnosis, care, and treatment, but also desired open discussions concerning these topics. Clarity and continuity were also important to patients, many of whom felt their opinions were often brushed aside. Communication is a central part of PCC, which involves active listening, the sharing of information, and deliberation surrounding treatment, each of which allow the individual to engage in their care (Santana et al, 2018). Face masks act as a barrier to purposeful communication, decreasing the effectiveness of PCC, and leaving patients feeling detached from their treatment as their views go unrecognised.
Respiratory infections are spread through droplets produced when an infected individual coughs or sneezes (Kohanski et al, 2020). Due to its easily transmissible nature and the sudden onset of this global crisis, there was an unexpected spike in cases which left hospitals struggling to support the masses of critically ill patients (Mahase, 2020). Hospitals were depleted in resources such as ventilators and PPE, and in many regions the number of patients outweighed the number of hospital beds available, impeding healthcare workers’ ability to deliver high quality care (Sen-Crowe et al, 2020). Not only was there a lack of essential equipment, but a shortage of healthcare employees also became apparent. The scarcity of nursing staff had been noted prior to the pandemic, with The American Nurses Association estimating shortfall of 1.1 million nurses in 2019 (Alipour et al, 2019). COVID-19 only magnified this shortage, forcing some countries to bring their final year students into the workplace early to support the demand, and some medical schools graduating their students early too (DeWitt, 2020).
As patient numbers increased, the strain placed upon nurses was amplified causing many to experience fatigue and burnout. Prior to the coronavirus outbreak, it was not uncommon for nursing staff to experience burnout due to the long working hours and night shifts, causing a decline in patient satisfaction (Vahey et al, 2004). However, studies have found that coronavirus has exacerbated the already demanding environment, increasing burnout with Sampaio et al (2020) reporting higher rates of depression, anxiety, and stress amongst nurses than the general public. They also discovered that in Portugal, since the start of the outbreak, public nurses who are contracted to work 35-hour weeks and private nurses who work a 40-hour week, ended up working a mean of 42 hours per week. In addition, Sagherian et al (2020) discovered that the pandemic led to an increase in fatigue amongst nurses, associated with poorer work performance, with those caring directly for COVID-19 patients experiencing the highest levels of exhaustion.
Evidence shows that overstraining the nursing workforce has a negative effect on quality of care and safety, suggesting that PCC is less likely to be implemented (Muabbar et al, 2020). Both the imbalance of staff-to-patient ratio and the high levels of fatigue contribute to time constraints cast upon nurses, another barrier to providing PCC. The fast-paced working environment, made worse by COVID-19, makes developing partnerships with patients and their families challenging and patient’s desires may become pushed aside (Moore et al, 2017). In order to alleviate the immense pressure placed upon healthcare professionals throughout the pandemic, steps should be taken to tackle the worldwide shortage of nurses (Varghese, 2021). By tackling this shortfall, nurses would have more time to implement PCC, putting each patient at the centre of their care, to ensure their needs are met, which in turn should increase patient satisfaction.
The pandemic has caused immense disruption to our daily routines, resulting in a decline in mental health. Mind (2020) found that 60% of adults and 68% of young people with pre-existing mental health disorders felt their mental health had worsened due to COVID-19. Of those who have never encountered mental health problems, 53% of adults and 57% of young people had a deterioration in their wellbeing. A study by Kumar (2020) highlighted a rise in depression, drug-use and suicidal behaviour since the beginning of the pandemic. However, severe psychological distress has also been detected amongst healthcare workers due to their vulnerable position making them more susceptible to coronavirus (Yang, 2020). The fear of infecting already at-risk patients has also caused employees to experience great anxiety (Nelson et al, 2020). A recent study by Greenberg et al (2021) assessed the mental status of those working in intensive care locations, discovering that 45% self-reported symptoms of PTSD, depression and anxiety with one in seven proclaiming thoughts of self-harm or suicide. However, the study had a number of drawbacks including the absence of participant demographics which could have influenced mental health. Furthermore, the self-reporting nature of the study may have contributed to response bias. Poor mental health can have detrimental effects, with repercussions likely to occur in a clinical working environment. Hennekam et al (2020) revealed that poor mental health adversely influences job performance, which can have serious consequences for patient safety.
As the demand for mental health services rises, research has concluded that there is serious underfunding in this sector, which is struggling to meet the publics’ needs, let alone those working in healthcare (World Health Organisation, 2020). PCC is concerned with putting the patient first, meeting all their healthcare needs to provide continuity of care, however the underfunding of mental health services may result in their mental wellbeing being disregarded. The decline in the psychological wellbeing of healthcare staff is another barrier to the application of PCC, as the impact on job performance could cause professionals to follow basic protocols and ignore the ideals that care should be holistic and tailored to each individual (Goodrich et al, 2008).
To conclude, COVID-19 has been detrimental to our lives on a global scale. Mental health has seen a significant decline, as individuals experience anxiety in contracting and passing on the disease, and the national lockdowns have resulted in an increase in loneliness and social isolation. Whilst the public has felt many of the effects of coronavirus, the healthcare system has taken the hardest hit. The peak of the pandemic saw a huge increase in the number of critically ill patients requiring treatment, which left hospitals depleted in both resources and staff. It is this imbalanced staff to patient ratio, the declining mental health of employees and burnout due to COVID-19 that contribute to reduced implementation of PCC, causing patients to feel their opinions surrounding treatment are disregarded. Furthermore, due to the widespread use of face masks, and the rise in telemedicine, communication between professionals and patients has suffered causing underdeveloped inter-professional relationships. PCC is crucial as it places patients at the centre of their treatment, presenting numerous benefits to clients and the healthcare system. Services should be aware of the long-term impacts of COVID-19 on the implementation of PCC, especially as the world attempts to recover from the pandemic.
Bibliography
Top of Form
Alipour, Z., Eskandari, N., Abbasi, M., Raisi, M., & Bakouei, S. (2019). Structural challenges in the health domain of the health system reform: A qualitative study. Journal of Education and Health Promotion, 8, 55.
Arabiat, D., Whitehead, L., Foster, M., Shields, L., & Harris, L. (2018). Parents’ experiences of family centred care practices. Journal of Pediatric Nursing, 42, 39-44. doi:10.1016/j.pedn.2018.06.012
Campagne, D. M. (2021). The problem with communication stress from face masks. Journal of Affective Disorders Reports, 3, 100069. doi:10.1016/j.jadr.2020.100069
Carbon, C. (2020). Wearing face masks strongly confuses counterparts in reading emotions. Frontiers in Psychology, 11, 566886. doi:10.3389/fpsyg.2020.566886
Desai, A. N., & Aronoff, D. M. (2020). Masks and coronavirus disease 2019 (COVID-19). JAMA : The Journal of the American Medical Association, 323(20), 2103. doi:10.1001/jama.2020.6437
DeWitt, D. E. (2020). Fighting COVID-19: Enabling graduating students to start internship early at their own medical school. Annals of Internal Medicine, 173(2), 143-144. doi:10.7326/M20-1262
Ekman, I., Swedberg, K., Taft, C., Lindseth, A., Norberg, A., Brink, E., . . . Sunnerhagen, K. S. (2011). Person-centered care — ready for prime time. European Journal of Cardiovascular Nursing : Journal of the Working Group on Cardiovascular Nursing of the European Society of Cardiology, 10(4), 248-251. doi:10.1016/j.ejcnurse.2011.06.008
Ferguson, L. M., Ward, H., Card, S., Sheppard, S., & McMurtry, J. (2013). Putting the ‘patient’ back into patient-centred care: An education perspective. Nurse Education in Practice, 13(4), 283-287. doi:10.1016/j.nepr.2013.03.016
Gajarawala, S. N., & Pelkowski, J. N. (2021). Telehealth benefits and barriers. Journal for Nurse Practitioners, 17(2), 218-221. doi:10.1016/j.nurpra.2020.09.013
Gameiro, S., Canavarro, M. C., & Boivin, J. (2013). Patient centred care in infertility health care: Direct and indirect associations with wellbeing during treatment. Patient Education and Counseling, 93(3), 646-654. doi:10.1016/j.pec.2013.08.015
Goodrich J & Cornwell J (2008) Seeing the Person in the Patient: The Point of Care Review Paper. King’s Fund, London.
Greenberg, N., Weston, D., Hall, C., Caulfield, T., Williamson, V., & Fong, K. (2021). Mental health of staff working in intensive care during covid-19. Occupational Medicine (Oxford), 71(2), 62-67. Doi:10.1093/occmed/kqaa220
Hentati, F., Cabrera, C. I., D’Anza, B., & Rodriguez, K. (2021). Patient satisfaction with telemedicine in rhinology during the COVID-19 pandemic. American Journal of Otolaryngology, 42(3), 102921. doi:10.1016/j.amjoto.2021.102921
Islam, M. S., & Kirillova, K. (2020). Non-verbal communication in hospitality: At the intersection of religion and gender. International Journal of Hospitality Management, 84, 102326. doi:10.1016/j.ijhm.2019.102326
Itamura, K., Rimell, F. L., Illing, E. A., Higgins, T. S., Ting, J. Y., Lee, M. K., & Wu, A. W. (2020). Assessment of patient experiences in otolaryngology virtual visits during the COVID-19 pandemic. OTO Open : The Official Open Access Journal of the American Academy of Otolaryngology–Head and Neck Surgery Foundation, 4(2), 2473974-2473974X20933573. doi:10.1177/2473974X20933573
JHU (2021), COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU), [Online], Available at: https://coronavirus.jhu.edu/map.html [Accessed on 10th March 2021]
Karina Cecilia, Arturo, Guadalupe, & Jorge. (2019). Evaluating mental workload for improved workplace performance Medical Information Science Reference. Retrieved from http://www.vlebooks.com/vleweb/product/openreader?id=none&isbn=9781799810544
Kumar, A., & Nayar, K. R. (2020). COVID 19 and its mental health consequences. Journal of Mental Health (Abingdon, England), ahead-of-print(ahead-of-print), 1-2. doi:10.1080/09638237.2020.1757052
Kuzma, A. E. (2020). Attitudes towards telehealth at the south burlington family practice Retrieved from https://scholarworks.uvm.edu/fmclerk/597
LEHULUANTE, A., NILSSON, A., & EDVARDSSON, D. (2012). The influence of a person‐centred psychosocial unit climate on satisfaction with care and work. Journal of Nursing Management, 20(3), 319-325. doi:10.1111/j.1365-2834.2011.01286.x
Mahase, E. (2020). Covid-19: Tighter restrictions imposed in the north of england as cases spike. Bmj, 370, m3066. doi:10.1136/bmj.m3066
Mahmood, S. U., Crimbly, F., Khan, S., Choudry, E., & Mehwish, S. (2020). Strategies for rational use of personal protective equipment (PPE) among healthcare providers during the COVID-19 crisis. Curēus (Palo Alto, CA), 12(5), e8248. doi:10.7759/cureus.8248
McCormack, B., & McCance, T. (2017). Person-centred practice in nursing and health care (Second edition ed.). Chichester, West Sussex, UK: Wiley Blackwell. Retrieved from http://bvbr.bib-bvb.de:8991/F?func=service&doc_library=BVB01&local_base=BVB01&doc_number=029048594&sequence=000001&line_number=0001&func_code=DB_RECORDS&service_type=MEDIA
Mheidly, N., Fares, M. Y., Zalzale, H., & Fares, J. (2020). Effect of face masks on interpersonal communication during the COVID-19 pandemic.Frontiers in Public Health, 8, 582191. doi:10.3389/fpubh.2020.582191
Mills, E., Savage, E., Lieder, J., & Chiu, E. (2020). Telemedicine and the COVID-19 pandemic: Are we ready to go live? Advances in Skin & Wound Care, 33(8), 410-417. doi:10.1097/01.ASW.0000669916.01793.93
Mind (2020) The mental health emergency: how has the coronavirus pandemic impacted our mental health? London: Mind. Available at: https://www.mind.org.uk/media-a/5929/the-mental-health-emergency_a4_final.pdf [Accessed on 14th May 2021]
Moore, L., Britten, N., Lydahl, D., Naldemirci, Ö, Elam, M., & Wolf, A. (2017). Barriers and facilitators to the implementation of person‐centred care in different healthcare contexts. Scandinavian Journal of Caring Sciences, 31(4), 662-673. doi:10.1111/scs.12376
Muabbar, H. Y., & Alsharqi, O. Z. (2021). The impact of short-term solutions of nursing shortage on nursing outcome, nurse perceived quality or care and patient safety. American Journal of Nursing Research. Vol. 9, no. 2: 35-44. Doi: 10.12691/ajnr-9-2-1
Nelson, S. M., & Lee-Winn, A. E. (2020). The mental turmoil of hospital nurses in the COVID-19 pandemic. Psychological Trauma, 12(S1), S126-S127. doi:10.1037/tra0000810Top of Form
Pattison, S., & Wainwright, P. (2010). Is the 2008 NMC code ethical? Nursing Ethics, 17(1), 9-18. doi:10.1177/0969733009349991
Sagherian, K., Steege, L. M., Cobb, S. J., & Cho, H. (2020). Insomnia, fatigue and psychosocial well-being during COVID-19 pandemic: A cross-sectional survey of hospital nursing staff in the united states. Journal of Clinical Nursing, doi:10.1111/jocn.15566
Sampaio, F., Sequeira, C., & Teixeira, L. (2020). Nurses’ mental health during the covid-19 outbreak: A cross-sectional study. Journal of Occupational and Environmental Medicine, 62(10), 783-787. doi:10.1097/JOM.0000000000001987
Santana, M. J., Manalili, K., Jolley, R. J., Zelinsky, S., Quan, H., & Lu, M. (2018). How to practice person‐centred care: A conceptual framework.Health Expectations : An International Journal of Public Participation in Health Care and Health Policy, 21(2), 429-440. doi:10.1111/hex.12640
Sen-Crowe, B., Sutherland, M., McKenney, M., & Elkbuli, A. (2021). A closer look into global hospital beds capacity and resource shortages during the COVID-19 pandemic. The Journal of Surgical Research, 260, 56-63. doi:10.1016/j.jss.2020.11.062
Vahey, D., Aiken, L., Sloane, D., Clarke, S., & Vargas, D. (2004). Nurse burnout and patient satisfaction. Medical Care, 42(2), II57-II66. doi:10.1097/01.mlr.0000109126.50398.5a
Varghese, A., George, G., Kondaguli, S. V., Naser, A. Y., Khakha, D. C., & Chatterji, R. (2021). Decline in the mental health of nurses across the globe during COVID-19: A systematic review and meta-analysis. Journal of Global Health, 11, 05009. doi:10.7189/jogh.11.05009
Wang, B., Liu, Y., Qian, J., & Parker, S. K. (2021). Achieving effective remote working during the COVID‐19 pandemic: A work design perspective. Applied Psychology, 70(1), 16-59. doi:10.1111/apps.12290
Williams, N. (2021) Working through COVID-19: ‘Zoom’ gloom and ‘Zoom’ fatigue. Occupational Medicine (Oxford), doi:10.1093/occmed/kqab041
World Health Organisation, COVID-19 disrupting mental health services in most countries, WHO survey finds; world mental health day on 10 october to highlight urgent need to increase investment in chronically underfunded sector. (2020, Oct 5,). African Press Organization
Wosik, J., Fudim, M., Cameron, B., Gellad, Z. F., Cho, A., Phinney, D., . . . Tcheng, J. (2020). Telehealth transformation: COVID-19 and the rise of virtual care. Journal of the American Medical Informatics Association : JAMIA, 27(6), 957-962. doi:10.1093/jamia/ocaa067
Yang, L., Yin, J., Wang, D., Rahman, A., & Li, X. (2020). Urgent need to develop evidence-based self-help interventions for mental health of healthcare workers in COVID-19 pandemic. Psychological Medicine, , 1-2. doi:10.1017/S0033291720001385